Chronic pilonidal disease requires reliably curative surgical intervention. The cleft-lift procedure is a novel approach offered at PTCNJ.
When a patient has had multiple abscesses, or has developed a chronically draining sinus tract, surgical removal of the diseased tissue is indicated. Historically, the so-called “pilonidal cystectomy” was wrought with wound breakdown, prolonged healing times, and high recurrence rates. Fortunately, a novel approach to the cure of pilonidal disease called the “cleft-lift procedure” has evolved. When performed by a specialist, the cleft-lift brings superior healing and a low risk of recurrent disease.
The cleft-lift finds its origins in a precursor operation conceived by Greek surgeon G.E. Karydakis in the early 1970’s. In the “Karydakis flap”, an elliptical incision was created that incorporated the entirety of the diseased intergluteal cleft, but was strategically offset several centimeters from the midline. This approach brought the sutured surgical wound to the side of, rather than within, the inhospitable cleft, in a microenvironment far more conducive to healing.
Karydakis Flap procedure
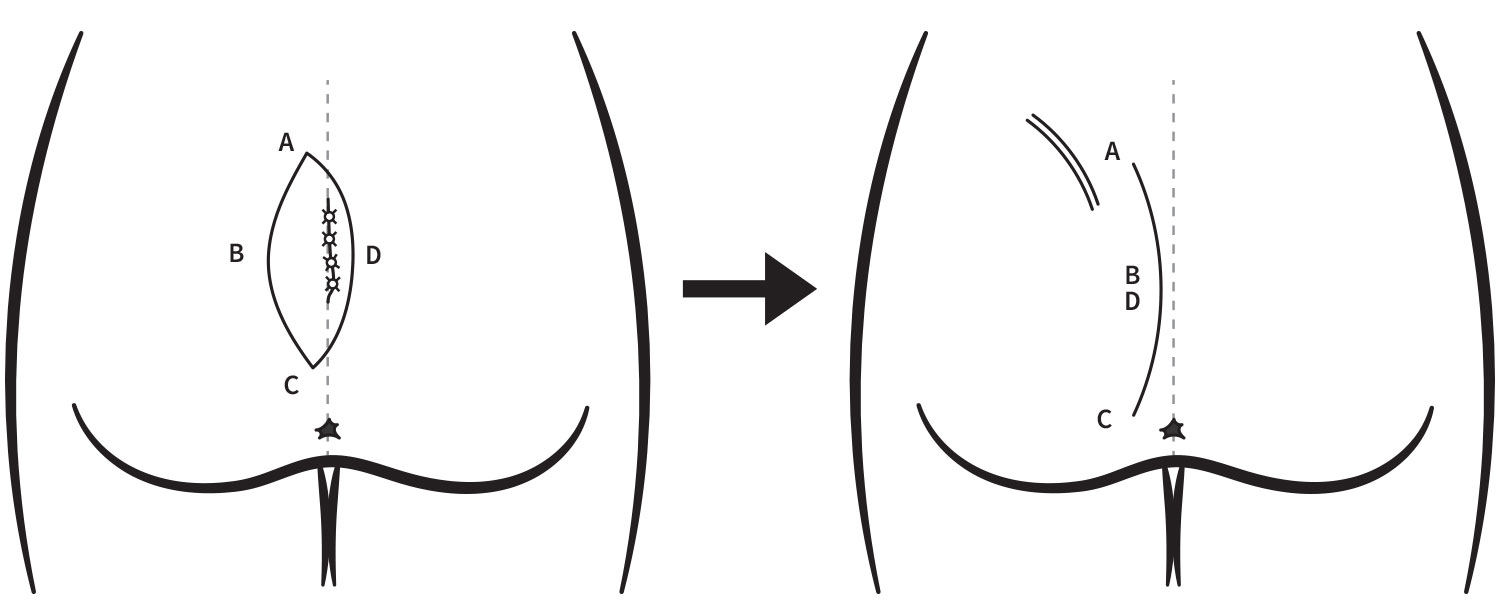
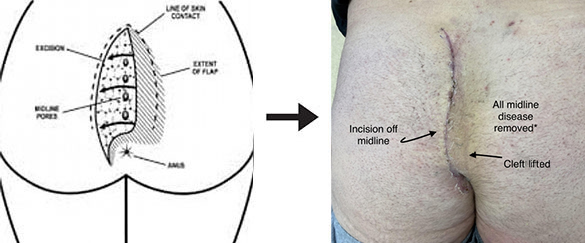
Building on the off-midline approach, American surgeon John Bascom further tailored the technique. He introduced the preoperative inscription of “safety lines”, the arcuate lines of gluteal skin contact seen when the patient is standing. These lines help define the incision and flap margins. Moreover, by modifying the tension in the closure, he added a shallowing or “lifting” of the cleft. This flatter cleft contour is the most important factor in recurrence risk reduction.
At PTCNJ, the cleft-lift procedure is performed in our ambulatory care center under general anesthesia. The duration of surgery is approximately 90 minutes. The resulting wound is closed in four absorbable suture layers over a small drain. Patients are asked to rest at home for 48 hours after the procedure. The drain is removed either at home by a family member or friend, or in our Center, at approximately one week following surgery. Stress to the operative site is avoided for 3 weeks. Full healing is seen between 3 and 6 weeks.
Frequently Asked Questions
General anesthesia, i.e. putting the patient “to sleep”, is the most common form of anesthesia used in the cleft-lift procedure. The secure airway into the trachea or windpipe used in general anesthesia conveys the greatest safety while the patient is in a prone position throughout pilonidal surgery.
There is minimal wound care following the cleft-lift procedure. The wound is fully closed with multiple layers of dissolvable sutures and skin glue. The incision may be safely washed with soap and water in the shower starting the first postoperative day and continuing on a daily basis thereafter. There is a drain left in place that must be emptied 2-3 times per day for about one week following this pilonidal surgery. The drain exits the skin at least 12 inches from the main incision, and the exit site is protected by a durable waterproof band-aid for the week. Once the drain is removed at one week, a new band-aid is required on the drain hole until a scab forms.
A properly performed cleft-lift results in a long scar extending from the top of one butt cheek down to the bottom tip of the tailbone. The scar has a gently curved lazy-‘S’ configuration. It is designed to be fully covered by the bottom piece of a two-piece bathing suit. We encourage hair growth to obscure the scar as desired. The cleft-lift, when properly performed, changes the contour of the gluteal region; stated plainly, the intergluteal crease, or butt crack, is literally lifted, i.e. made much more shallow and flat. This is a critical factor in the longterm success of the operation. Many describe an appearance of having “lost” a segment of the crack. This change is not noticeable under casual clothes. If one is uncomfortable with these cosmetic changes, strong consideration should be given to our minimally invasive pilonidal cyst treatment.
There are 4 subgroups of our tailbone area pilonidal patients for whom gluteal cleft-lift is indicated: those with recurrent (≥2) abscesses requiring drainage, those with one or multiple chronically draining sinus tracts, those with nonhealing surgical wounds from previously failed pilonidal surgeries, and select patients with chronic tailbone pain or coccydynia.
Patients are encouraged to wear loose-fitting comfortable clothes in the weeks following this pilonidal surgery; sweat pants are optimal, particularly those with a pocket to discreetly hold the drain bulb. Jeans and similarly fitted pants should be initially avoided but can gradually be resumed by the third week following surgery.
Exercise is limited to moderate walking (≤ 2 miles/day) for the first week after surgery. Once the drain is removed at one week, more strenuous cardiovascular exercise such as running and swimming may be introduced. When full wound healing is achieved, somewhere between 3 and 6 weeks after surgery, exercise of all kinds is fully unrestricted, including distance biking, jogging, horseback riding, and all weightlifting including squatting.
Following pilonidal cystectomy, you should plan for a 2-3 day absence from work or school. If your duties mandate prolonged sitting, or heavy lifting, 1-2 weeks of leave is preferred. If only an incision and drainage has been performed, a one day absence should suffice.
The gauze bandage on the wound is removed after 48 hours and the wound is then cleansed with soap in the bath or shower. The wound is patted dry, and then left unbandaged, with the exception of the drain sponge and the small glued tape strips The strips will naturally fall off in several weeks, and may become wet in the bath or shower.
A drainage tube is left deep to the wound to prevent fluid accumulation. It exits the skin at least a finger’s length away from the main incision at the upper aspect of the opposing buttock. This is connected to a self-expanding bulb, which is often safely pinned to the underwear. The drain is emptied several times a day. It is generally removed at home by a family member at one week following surgery.
Sitting is encouraged the day after cleft-lift procedure. We recommend patients sit on a cushioned yet supportive surface for as long as tolerated. This helps express seroma fluid from the drain in the week following surgery. We also recommend patients sit the day after the pit-picking procedure.
Pain is generally not severe following pilonidal surgery. In the cleft-lift procedure specifically, we perform an ultrasound-guided nerve block of the tailbone area just prior to incision. The numbing effect achieved with this lasts 48 hours. We supplement this with routine oral naproxen and prescription pain medication as needed. With this tri-modal approach to pain, patients find pain quite manageable. Patients can get comfortable in certain positions and can resume light exercise within several days.
There are two effective surgeries for a pilonidal sinus. The far most effective surgery is the cleft-lift procedure in which the sinus is removed as the gluteal cleft is made more shallow. The latter objective permanently disrupts the mechanism that drives the disorder. With the cleft-lift, fast wound healing and low recurrence rates are the rule, provided the procedure is performed by a dedicated pilonidal surgeon. For patients wishing a more conservative approach with a quicker recovery, the pit-picking procedure can be performed. In the pit-picking procedure, we remove the sinus opening and simultaneously clean and debride the midline pits, sometimes achieving prolonged periods of disease dormancy.
Automobile travel is permitted immediately following pilonidal surgery of any kind including the cleft-lift procedure. Travel of this type should be limited to 6 hours in a day. With regards to timing, the day or evening of the surgery is preferable to the day after the surgery because residual sedation allows for better patient sleeping during the ride. Reclining in a passenger seat or laying supine on connected back seats is recommended. With regards to air travel, it is recommended that flights not be scheduled until at least two days following surgery
CONTACT US TODAY!
Contact us today and let us help you leave your pain behind.

